Overview: What is melasma?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
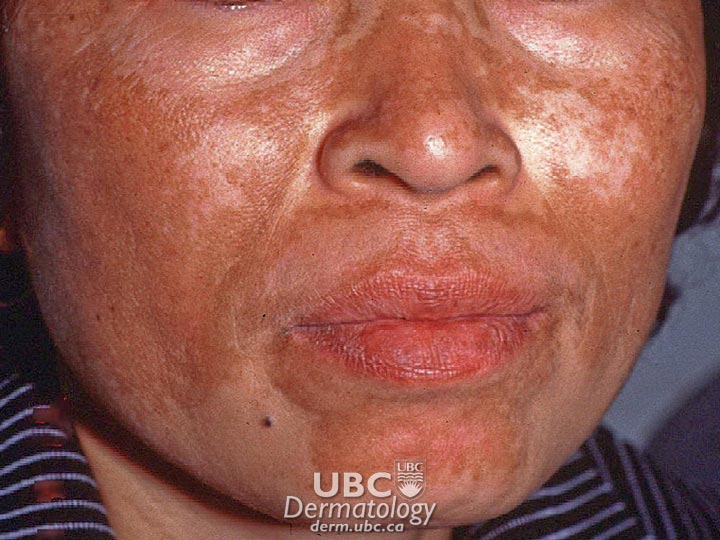
Melasma is a skin condition in which dark patches develop on both sides of the face. The distribution of patches is symmetrical and most commonly appears on the forehead, cheeks, nose, upper lip and chin. It will not spread to other areas of the body and it is not contagious.
The patches are caused by increased amounts of melanin (skin pigment) in the skin. The excess melanin may be located in the top layer of the skin (epidermis), in the middle layer (dermis), or both. The location of the pigment is an important factor when considering treatment options.
The condition may run in families and occurs mainly in women of child-bearing age. The condition has also been called the “mask of pregnancy,” as it tends to appear during pregnancy. After pregnancy, the mask often fades but may recur with subsequent pregnancies.
Melasma is also more common in people with darker skin types, especially Hispanics and Asians.
 melasma-1
melasma-1  melasma-2
melasma-2
Causes
Though the mechanisms that trigger melasma are still under investigation, there appears to be a direct relationship with female hormonal activity, as the condition is common among women who are pregnant and those who use oral contraceptives. Certain medications or cosmetics may also cause skin darkening. Sometimes a thyroid gland dysfunction can contribute to the condition.
The most important cause appears to be sunlight exposure. The ultraviolet radiation in sunlight stimulates the overactive melanocytes to produce more melanin than the normal melanocytes in surrounding skin. Further exposure of the affected patches can cause additional darkening and, during treatment, can cause potentially successful treatments to fail. Some individuals may have a genetic susceptibility to developing melasma. More than 30 per cent of people with melasma have a family history of it, and there are reports of the condition affecting identical twins but not other siblings under similar living conditions.
In general, the condition tends to persist, though treatments are available to gradually lighten the darkened skin.
Diagnosis and Treatment
Your doctor will diagnose the condition through a physical examination and a medical history. A thyroid test may be conducted to rule out thyroid disease. Examinations are often done using a Wood’s lamp or light, which shines ultraviolet light onto your skin. This will help your doctor identify whether the affected melanin is in the dermis or epidermis. (However, this type of light cannot be used accurately on people with dark brown skin.) Your doctor may also ask if you experienced any inflammation before the dark patches appeared, have been exposed to chemicals, or have been taking any medications that might cause pigment deposition.
Your doctor will also want to rule out other conditions that can cause the patches, such as menopausal changes, certain types of ovarian tumours and disorders such as Addison’s disease.
Melasma cannot be cured, and many cases require no treatment at all. For example, the melasma associated with pregnancy usually fades slowly after delivery; similarly, dark patches will fade eventually after discontinuation of oral contraceptive use. It will likely recur upon subsequent pregnancies or when restarting use of the contraceptive.
Cases of melasma where the melanin is in the deeper layer (dermis) are slower to resolve than cases in which melanin is restricted to the epidermis, as pigment deposited in the skin’s deeper layers cannot be physically removed. Treatment of dermal melasma aims to prevent the melanin in the dermal layer from being replenished. This results in very slow fading of the pigmented areas. In all cases, strict avoidance of sunlight is crucial to successfully resolving melasma and preventing resistant cases or recurrences.
Treatments for melasma include:
Topical Depigmenting Agents
- Hydroquinone (HQ) is a chemical that interferes with the process that melanocytes use for producing melanin. Formulations with higher amounts of HQ are more effective than those with lower amounts; however, adverse side effects increase with drug concentration. Side effects include skin irritation, sensitivity to light, and hyperpigmentation (darkening of the skin), some of which may be irreversible. Tretinoin (trans-retinoic-acid) is thought to increase the turnover of skin cells in the epidermis, which limits the transfer of melanin to the skin. Tretinoin is often used in combination with HQ as response is slow when tretinoin is used alone. Its side effects include skin irritation, temporary sensitivity to light and hyperpigmentation.
- Azelaic acid reduces melanocyte function. Unlike HQ, azelaic acid seems to target only hyperactive melanocytes. Normal melanocytes in light skin will not be affected. The primary adverse effect is skin irritation.
- Other depigmenting agents under study include 4-N-butylresorcinol, phenolic-thioether, 4-isopropylcatechol, kojic acid, and ascorbic acid.
Chemical and surgical peels
Chemical peels, microdermabrasion, and laser surgery have all been used to remove the layer of skin with the malfunctioning melanocytes. Results are obtained quickly but are unpredictable and may be temporary, as the melanocytes on the new skin may also malfunction. Such procedures can also irritate the skin, which can worsen melasma. Some physicians combine mild exfoliation with topical depigmenting agents. A number of studies have found this to be safe and effective.
Coping and Support
Melasma does not impact a person’s overall physical health. However, people with the condition may feel embarrassed, depressed or anxious due to their skin’s appearance. These feelings may lead to social isolation and loneliness and can be addressed by speaking with a psychologist.
To manage the physical symptoms of melasma, some people choose to cover the darkened patches with cosmetics. To prevent further damage, people with the condition must use sunscreen, even on cloudy or hazy days. A sunscreen that has a rating of 30 SPF or higher and that protects against both UVA and UVB rays is recommended. Some people with melasma use tanning beds in an effort to “even out” the appearance of their skin; however, this does not work, and tanning beds must be avoided as they can make the condition worse and have other dangerous side effects.
Symptoms
The symptoms of melasma include dark, irregularly shaped patches on sun-exposed areas of the face. Tan to brown patches indicate that the majority of pigment is in the epidermis (the outer-most layer of skin visible to the eye); blue or black patches indicate that the majority of pigment is in the dermis (the middle layer of our skin).
The distribution occurs in one of three patterns:
- centrofacial (across the centre of the face)
- malar (over the cheeks)
- mandibular (over the lower jaw)









